
No practicing physician could confute that smoking is one of the leading causes of morbidity and mortality worldwide.(1) Indeed, smoking in every form is detrimental for health in general, and in particular for cardiovascular well-being, thus representing a worthy enemy for any caregiver.(2) Despite momentous successes in our global fight against smoking, there remains a lot of room for further improvements.(3) This need for ongoing efforts in fighting smoking in every form and in every setting is well reinforced by the latest report from the Global Burden of Disease (GBD) Study, just published in the European Journal of Preventive Cardiology.(4) In this poignant analysis, leveraging information on 369 diseases and injuries and 87 risk factors around the world from 1990 to 2019, as well as comparative risk assessments for 204 countries and territories, Khan Minhas and colleagues investigated the trends in cardiovascular disease burden attributable to smoking for 30 years. Measures of interest were unadjusted death counts, disability-adjusted life years (DALYs), age-standardized mortality rates (ASMR) per 100,000 people, and age-standardized DALY rates (ASDRs) per 100,000 people.
While unadjusted estimates suggested a progressively increasing toll on cardiovascular mortality and morbidity due to smoking over the decades, more refined analyses capable of taking into account the effect of time and age within populations showed exactly the opposite. Remarkably, all the above adjusted indicators yielded significant decreases in the burden of smoking on cardiovascular disease, in general terms and also when focusing on individual cardiovascular conditions being analyzed (i.e., aortic aneurysm, atrial fibrillation, atrial flutter, ischemic heart disease, peripheral artery disease, stroke). For instance, ASMR decreased from 57 in 1990 to 33 in 2019 (a 42% reduction in relative terms), and ASDR went from 1435 in 1990 to 854 in 2019 (a 40% reduction in relative terms). Just to translate this figure into a tangible estimate, a 24 absolute decrease in ASMR such the one found by the GBD Investigators would translate into 528 fewer deaths in a city such as Paris (assuming a population for such a place of roughly 2.2 million inhabitants). These figures clearly represent a major success and a reason for celebration. Yet, we should not fool ourselves: the glass is half full, but also half empty. First, decreases were more evident for men, but less so dramatic for women. Furthermore, people in lower socio-demographic index strata displayed less benign reductions in smoking burden, and this held even truer in countries with less developed economies.
Evidently, we need to compliment ourselves for our recent successes in the global fight against smoking, but at the same time we should continue to proactively fight this veritable plague, while applying evidence based interventions capable of fostering smoking cessation and preventing smoking inception (Figure 1).(5) Moreover, research to improve our understanding of the reasons and subtleties of smoking dependence should continue, and further efforts should be implemented on testing and refining novel tools and approaches to progressively minimize the global cardiovascular impact of this deadly habit.(6) Indeed, success against smoking will translate into many additional benefits, including reduction in the burden of cancer and lung disease.
Figure 1. Evidence-based strategies that can be implemented, alone or in combination, to continue our efforts for smoking cessation.
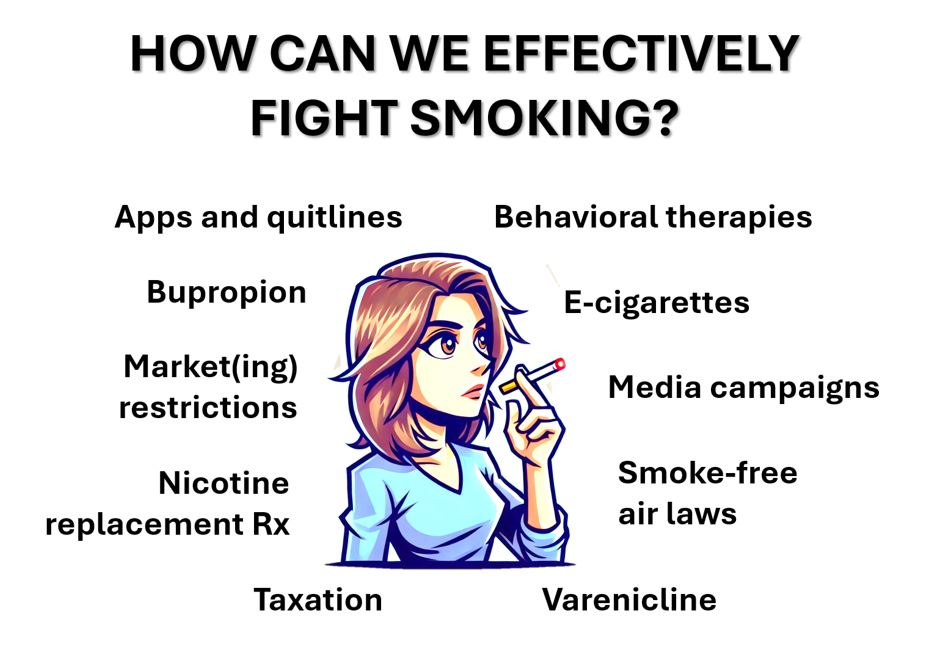
Source: Created by Giuseppe Biondi-Zoccai
Note: The content of this article reflects the personal opinion of the author/s and is not necessarily the official position of the European Society of Cardiology.